



🎧You Discover What It Means to Be Self-Directed | Chapter 9

🎧 Listen to Sarah read this chapter above or on Spotify:


Sunlight breaks through the clouds and comes in Dr. R’s office window. On the street below, rain soaks the pavement. The two together seem wrong: sun, rain.
I face him and take in his encouraging smile. His white shirt is perfectly crisp. I try to smile too, then glance back at the sunlight and the wet pavement. Without looking at him, I say, “I don’t want to change my meds—ever,” hearing the tremor in my voice. I’m still wrecked—shaky, cold-sweaty, brain-zapping—from having tried to go off my medications.
This is my second mistake in moving toward recovery from mental illness. Before that, I’d linked recovery to “normalcy” believing I shouldn’t be in therapy. It seemed obvious: “normal” people don’t need therapy or take psychotropic drugs; recovered people shouldn’t either.
If I’d had the guidance of Dr. R or someone who’d recovered, they’d have told me how wrong I was. Some people have been on medication for so long that their bodies are dependent. Withdrawal had already brought me to the brink of ending my life twice; this time, it brought me close enough to vow never to try to go off my meds again.
I’ve come up with a new strategy. Changing my medications—going off one to try another, upping the dosage of this one, lowering the milligrams of that one—has only complicated my mental health struggles. When new drugs and dosages are changed and changed again, it’s impossible to know what helps and what harms, how much is the drugs and how much is the result of mental illness. I now have a baseline where the side effects are minimal. Having the drugs in my system is my normal. And it doesn’t mean I’m sick.
Dr. R nods. “Okay. Any reason you don’t want to ever change your meds, ever again?” He says this slowly.
I tell him my baseline theory. Whatever painful emotions, troubling thoughts, and unwanted behaviors come, I won’t answer them with medication changes.
Dr. R nods, Got it. Not a problem. “Ultimately, it’s your treatment.”
I look out the window onto Michigan Avenue at the cars streaming through the stoplight. It’s hard to make that decision and have him agree. Until then, I did as my doctors told me to do. Should I really be the one to determine what’s best for me?
*
Had I known about the principle of shared-decision making in psychiatric treatment, I may not have hesitated. For two decades, studies have shown that treatment tailored to patient preferences is associated with
greater engagement in treatment,
an improved therapeutic relationship,
increased patient satisfaction, and
improved outcomes of care.1
That doesn’t mean a clinician isn’t involved, just that treatment is aimed at recovery, not maintenance as it is now, i.e., we’re given the chance to do more than just “manage” our symptoms. And treatment isn’t determined by the clinician and accepted by the patient. The clinician may make suggestions, but the patient is in charge.
I know how that may sound. I can imagine how it would have sounded to my mother during my worst times. How could I—chronically suicidal and unable to live independently—really determine my own treatment?
Maybe I couldn’t have been in charge while in crisis. Someone in a psychotic or manic or suicidal or depressive episode may not have the inner resources to do that.
Self-determined treatment takes that into account. It involves deciding what we want when we’re in remission, i.e., stable, or even before we ever walk into a mental health professional’s or GP’s office. A mental health advance directive.
It might come in the form of the shared decision-making card developed by Maria O’Connell and Janis Tondora, both professors of psychiatry and researchers in the Program for Recovery and Community Help at Yale School of Medicine.
On the shared-decision making card, patients mark the three most important things they want from their clinician and treatment, e.g., obtain medication that works for me, ask who I want to be involved in my care, respect my time, be informed of all options for treatment, receive an accurate diagnosis, not be rushed.
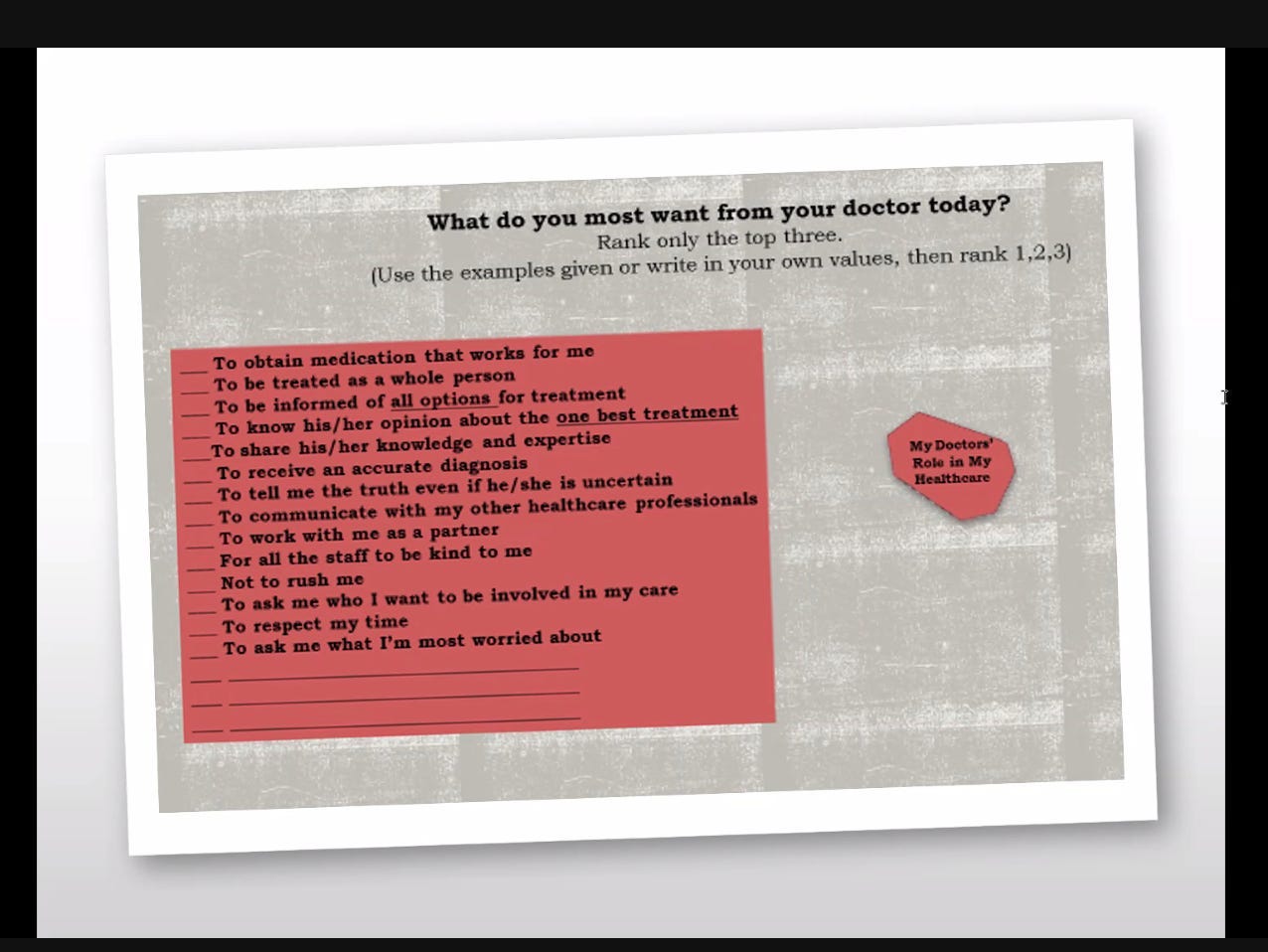
O’Connell and Tondora stress how important this could be for someone in crisis. And think how it could serve young people—or any of us—in preparation for when we have to articulate our mental health needs.
A card like this—or a document—can only help our clinicians. We ask so much of them. They can’t be everything and all to us. They can’t know what we need if we don’t tell them. To get the best treatment, we have to create our own care.
*
Shared-decision making likely wouldn’t exist as a principle if not for the Recovery Movement. Unfortunately, the day I sat in Dr. R’s office, I’d never heard of the movement. During my twenty-five years in the mental health system, no one mentioned it. I was in and out of hospitalization programs, in and out of psychiatrists’ and therapists’ and GPs’ offices, and it never came up. I’d learned about Sigmund Freud and cognitive behavioral therapy and second-generation anti-psychotics and a lot of misinformation about the supposed chemical imbalance theory of mental illness (which would turn out to be and always have been totally false) but nothing about the legions of people and groups in the Recovery Movement who have been trying to tell us that we can, in fact, recover from mental illness, even serious mental illness, and psychiatric disorders if we receive the right treatment.
The right treatment depends on self-directed care. Since the 1970s, the Recovery Movement has focused on patients’ rights. By then, the government policy to close psychiatric institutions and replace them with community mental health centers had failed. Only a third of the promised mental health clinics had been built, inpatient beds were scant, and funds meant for community services ended up mired in bureaucracy or wasted on maintaining the remaining dilapidated institutions.
During this period, a group of strong-willed ex-patients set out to abolish the mental health system, liberate patients who’d been abused and mistreated in psychiatric institutions, and create a new system of care. The movement’s core members took their cues from the civil rights movement, including Black Power and gay pride, coining the term insane pride. Various groups organized the movement, including the Insane Liberation Front based in Portland, Oregon (1970); the Mental Patient’s Liberation Front in Boston (1971); the Mental Patient Liberation Project in New York City (1971); and the Network Against Psychiatric Assault in San Francisco (1972).
The movement went by various names: the Mental Patient Liberation Movement, the Psychiatric Survivor’s Movement, and the Ex-Patients Movement. In most cases, non-patients weren’t allowed. Often, membership was limited to patients who’d been hospitalized; those who’d received outpatient care didn’t qualify. Mental health professionals were occasionally granted a tangential connection to some groups.
At first, they sought to overturn psychiatry, not improve the current system. To them, psychiatry was a capitalist industrial complex. Reform wasn’t possible, only abolition. The slogan “Nothing about us without us” sent the message that mainstream psychiatry’s days were numbered.
The movement’s leaders focused on fighting for the rights of “psychiatric prisoners” based on their own experiences. Howie Geld—a.k.a., Howie the Harp, a nickname given in honor of his love for the harmonica, which he learned to play while institutionalized after a suicide attempt as a teenager—ran the Mental Patients’ Liberation Party and eventually founded the Community Access mental health center in New York City. Leonard Roy Frank, a one-time graduate of the Wharton School of Business who was hospitalized for paranoid schizophrenia and subjected to thirty-five rounds of ECT treatments and thirty-five psychosurgeries, was one of the primary writers on the staff of Madness Network News, the movement’s media outlet, which published the views of ex-inmates and psychiatric survivors. Other pivotal activists included Sally Zinman, Dan and Su Budd, Tom Wittick, Dorothy Weiner, Tanya Temkin, and Rae Unzicker.
Judi Chamberlin, a self-described “crusader,” was the movement’s most visible spokesperson. When she was in her twenties, she sought treatment for postpartum depression. After her first office visit, a psychiatrist quickly prescribed her two potent antipsychotics: Thorazine and Stelazine. She didn’t improve. The psychiatrist said she should be hospitalized. Over six months in 1966, she went in and out of six New York hospitals. She went into treatment a housewife suffering from depression and came out a patient diagnosed with “chronic schizophrenia with homicidal and suicidal tendencies.”
With the help of a psychologist and finding purpose in the Women’s Liberation Movement, she recovered and joined the cause for patients’ rights.
Her 1978 book On Our Own: Patient-Controlled Alternatives to the Mental Health System called for a system in which people with mental illnesses weren’t “passive recipients of institutional ‘care’” and instead were encouraged “to see the strong and positive aspects of themselves as they, in turn, help others.” As Dan Fisher—a protégé of Chamberlin’s and a clinical psychiatrist who healed from schizophrenia and has been working in the Recovery Movement since its inception—told me, if the Diagnostic and Statistical Manual (DSM) is psychiatry’s “bible,” On Our Own was and is the Recovery Movement’s “bible.”
The Recovery Movement made history-making strides throughout the 1970s. Privately funded community centers run by those with lived experience of mental illness started across the country: Horizon House in Philadelphia, Fellowship House in Miami, The Green Door in Washington, D.C., and Thresholds in Chicago. These centers managed to keep their doors open without proper funding or government support, so determined were they to give people the ways and means to heal.
Fifty years ago, those in the Recovery Movement knew that healing occurs when patients are treated as human beings, play a role in their treatment, are given the opportunity to recover, and aren’t assumed to be suffering from chronic conditions. As Phyllis Vine points out in Fighting for Recovery: An Activists' History of Mental Health Reform, the term chronically mentally ill riled those in the movement.
Chronic typically means persistent but is often understood to mean lifelong. As Stephanie Bernell and Steven Howard, researchers in public health, show, there is no uniform definition of chronic, not even within the Department of Health and Human Services. Some say it’s any condition lasting longer than three months, some longer than a year, some “of long duration,” and some simply an illness that “cannot be cured.”
The general idea behind the term is that our conditions are hopeless. They aren’t. Not when we dictate our own care. Those in the Recovery Movement knew this, as do so many today.
If you haven’t already purchased access to Cured for $30—about the price of a hardcover book—you can do so here:
» Continue to Chapter 10.
Find resources for mental health recovery.
Enjoying ‘Cured’? Read the prequel, ‘Pathological’ (HarperCollins):

Andersen & Urban, 1999; av a Pinikahana, 2007; Donovan, 1995; Greenfield, Kaplan, & Ware, 1985; Greenfield, Kaplan, Ware, Yano, & Frank, 1988; Hibbard & Greene, 2013; Kaplan, Greenfield, & Ware Jr; 1989; LeBlanc, Kenny, O'Connor; & Legare, 2009; Stacey, Carley, Ballantyne, Skrutkowski, & Whynot, 2014.